
NANOSPRESSO and the Future of Personalized Nanobrewed Therapies
Pharmacists as baristas

They’ve done it. Or are planning to. They’ve turned the multicomponent mRNA therapeutics precision manufacturing into a Nespresso machine. Seriously. A personalized push button mRNA/siRNA/CRSPR made to order in your hospital pharmacy with the pharmacist as your barista.
This post in a bit of a personal one, since I worked and was a consultant for a hospital pharmacy that lived in the early 90s, that I pushed and pulled to 2015 standards. So I want to give my personal view on this new paper as a hospital pharmacist, not as an independent researcher this time around.
Introducing the NANOSPRESSO Personalized LNPs
See our favorite Canadian LNP pioneer is involved? Of course he is. This is a REAL paper. You can find it here. June 2025 in Frontiers in Science LEAD ARTICLE.
This is a device they are developing that miniaturizes the microfluidic and sterile filtration, fill and finish steps of making an mRNA or siRNA or CRSPR therapy for a single N of 1 therapy at the hospital bedside.
It is supposed to “democratize” gene therapy by using current hospital exemptions for compounding and letting the hospital pharmacists make individual gene therapy products. As if making multi-drug individualized hazardous chemotherapy wasn’t enough. Or pediatric total parenteral nutrition. It is not as if pharmacists are not capable of doing this. They are. And they wont need that much training.
But HOLY TOLEDO WHAT ARE THEY THINKING? Even if I thought mRNA and gene therapies with those LNPs were the best thing ever, this idea is fraught with challenges. Why are they doing this?


Ahhh, personalized gene therapy is too EXPENSIVE for the pharmaceutical companies, so we will just download that to hospital pharmacy, and the hospital sector to provide these therapies.
The memes write themselves.

Figure 1. The NANOSPRESSO System:Personalized Therapy at the Touch of a Button
Prototype model for microfluidic bedside compounding.
Selectable programs: mRNA / siRNA / CRISPR. Final product dispensed directly into sterile 10 mL syringe. QC pending. (made by Grok after much poking and proding to get what I wanted, lol)
Personalized Medicine, Meet the Latte Machine
So here is their premise. Nucleic acid production that is:
local
modular
for orphan diseases
It will have a “cartridge” of the specific personalized nucleic acid, be it mRNA, siRNA or CRSPR or some kind, and another “cartridge” for the lipids.
Is THAT GMP? A bedside biotech coffee pod? Are those lipids stored and free of N-oxides and adducts? Is that mRNA free of plasmid DNA? The siRNA without dsRNA and those CRSPR pods are guaranteed endotoxin free? You could ask for the “organic” filters without endotoxin perhaps. But who would know?
So instead of centralized vaccine factories and billion‑dollar GMP facilities, a hospital pharmacy could produce on‑demand personalized nanomedicines for rare diseases. Load one capsule with lipids, another with nucleic acids, slide them into the NANOSPRESSO, and out comes your patient’s bespoke RNA therapy — “high quality, flexible, and democratized.”
This paper has all the buzzwords.
SUSTAINABLE, PATIENT-CENTRIC, COST-EFFECTIVE, MODULAR and of course my favorite. AGILE.
When you see these words. RUN!
The Irony of it all
I have spent the last 5 years studying and writing about how astonishingly COMPLEX the manufacturing and science behind the mRNA vaccines are, and now they are being simplified for bedside use. Oh the irony.
I mean my techs were fantastic, and pharmacists CAN do this with the proper training, but HOW can we do standardized quality control when the quality control people (ie the USP which we follow in hospital) haven’t even finalized the quality metrics, methods and criteria for mRNA therapies? How will this be done in a “brew your own RNA” environment? How?
We know that centralization at Big Pharma is problematic and decentralization is something I am usually in favour of, but this is decentralization without the appropriate safety net. I bet, because this is an N-of-1 type situation, then quality control is considered less of an issue under current regulatory hospital guidelines. Because you’re are not bulk compounding (which would have it’s own set of quality measures to follow), quality control would be process only. Yikes.
Quality Control, Now with Froth
So in a previous life, I helped set up a spanking new clean room for hazardous compounding (ie CHEMO) as well as bulk compounding of sterile products, like antibiotics, epidurals and the like. There is a LOT to this. Really, unless you’ve worked in a hospital pharmacy you have no clue of the amount of documentation and the regulatory burden. It is very similar to what Pharma has to do in fact. For one simple chemotherapy set up, it takes about 4 hours of prep work to document and set up including the right type of IV lines, the right type of IV bag, syringe etc. Every step is photographed so it can be traced, everyone who touched the order, or paper, or any part of the drug is documented.
So the setup for one mRNA macchiato with froth would probably take at least 12-16hrs or more prep time. So where are the people to CHECK THIS. How are we going to take a picture of every step? Clearly the main barrier to pharmacogenomics was that pharmacists didn’t have enough kitchen appliances in hospital pharmacies (irony: we are NOT ALLOWED TO EAT in the hospital pharmacy and NO COFFEE MACHINES ALLOWED AT ALL. We would sneak in our coffee cups but they all had to be sequestered in one tiny area away from all the compounding, like in the managers office…)

Figure 2. Sterile Compounding of a Single‑Origin mRNA Shot
Pharmacy technician operating the NANOSPRESSO system under USP <797> clean‑room conditions. Precise dosing ensured via calibrated balance and deep personal disbelief. (Thanks Grok)
The Reality is Sterility, Documentation, and the Dull Work of Safety
Sterile compounding is tough and disciplined. You have aseptic tech, airflow validation, operator qualification, and full traceability. The idea that a hospital pharmacist could “assemble nucleic acid nanomedicines bedside” with the same ease as a latte ignores roughly 90 percent of the quality system holding modern pharmaceuticals together.
Manufacturing is not the same thing as compounding. Manufacturing is proactive engineering: validation, monitoring, environmental metrics, multi‑stage stability studies. Pharmacists USED to do this, my first hospital pharmacy had a state of the art manufacturing lab, with HPLC, mass spec, the works. But they got rid of it all because we were MANUFACTURING and only Pharma could do this. And they didn’t want to pay the salary of this brilliant, but quiet and shy manufacturing pharmacist. Now they want to return to the way it was 30+ yrs ago?
And we’re not talking about simple antibiotics and long term sterility and stability of known molecules. These are LNP‑encapsulated nucleic acids that interact with cell membranes and immune receptors. They require particle‑size analysis, quantification of RNA/siRNA/DNA, encapsulation efficiency verification, nuclease stability testing for each bespoke product. Biological testing, not small organic molecules. But sure, go ahead and “insert cartridge, press start.” Holy Toledo. Since this is unpractical and expensive, they will likely SKIP the QA part. Just watch.
This is Decentralization Without Accountability
The paper’s authors frame NANOSPRESSO as liberation from Big Pharma’s centralized control. Ok fine. Central control creates monopolies, increased costs, and those really awful Byzantine supply chains. But decentralization without structure will likely end up in chaos.
Every pharmacist remembers the 2012 NECC compounder disaster in the US when “just‑in‑time local production” turned into fungal meningitis for 750 patients. That wasn’t a failure of centralization; that was a failure of oversight and quality control manufacturing. In Ontario we had something similar happen with underdosing of chemotherapy which spurred a whole slew of regulations, training, accreditation standards and the like.
Now scale that to RNA therapeutics with microbubble precision equipment and no lot testing. Because there is no “lot” because each lot has only ONE vial. What would you compare it to? So how to ensure quality? Just make sure the size is OK? the encapsulation rate ok? Filtered properly? That’s it? Each hospital would become its own micro‑manufacturer. Regulators could never standardize safety data across hundreds of “bedside biotechs.” Who would be accountable? You guessed it, the pharmacist. Not the hospital, not biotech, not the government.
And let’s be honest. The endgame here is obvious: push manufacturing costs downstream and liability upstream. Hospitals pay for the hardware and personnel; industry supplies the products and collects licensing fees. Outsourcing to hospital pharmacies under the hospital pharmacy exemption. The provincial governments will LOVE this because it saves costs. And they sound INNOVATIVE, AGILE and all the buzz words.
Also unspoken is the resource fantasy. Hospital pharmacies are chronically understaffed. I have never worked in a fully staffed hospital pharmacy in my entire career. Never. Cleanrooms are over‑scheduled. And the techs don’t get paid for overtime, yet often do so for a patient for their chemotherapy. Budget lines for equipment evaporate annually. Many hospital pharmacies are cramped, old and in the basement. Where, exactly, does this bedside nanolab live? In the corner next to the pneumatic tube?
It’s not that pharmacists couldn’t handle this technology. It’s that none of the people proposing it have ever asked what we already do or how hard it is to do it consistently day after day. Oh sure, this will only be at those specialized hospitals, likely pediatric ones to start. And they will be sufficiently resourced to start. But for cancer? Chronic diseases? For crying out loud, I even saw a paper that was studying mRNA gene therapy for weight loss.
The Renaissance “They” Keep Promising
The authors close with lyrical optimism aka a snow job, lol. A “renaissance” of pharmacists reclaiming their artisanal heritage through personalized gene therapy production. It’s a sweet image: the apothecary re‑imagined through nanotech, the marble mortar replaced with a microfluidic chip. Back to my brilliant manufacturing pharmacist of old. That way AI can’t get rid of us, will be the hook. I can see it all now.
But in my view it is the hospital pharmacists independent clinical judgment that matters more than software prompts, when pharmacists are trusted as scientists, not operators of someone else’s device. Or are seen as the plumbers of health care. Or get called a building (inevitably we get called PHARMACY, not the pharmacist, not our name, no we get called the building). Seriously.
Give us the autonomy to challenge unsafe protocols and not go through layers of hospital administration who often have very little clue, to question unsafe gene therapies (and not get fired!) to interpret complex pharmacogenomic interactions, to manage therapy holistically, then we’ll be in a renaissance. Until then, we’re just baristas for biotech. Please don’t let that happen.
☕️ Final Shot/Summary
I genuinely admire the spirit and idea behind NANOSPRESSO: decentralize innovation, provide personalized care, take medicine out of fortress factories and closer to patients. Have the pharmacist more directly involved. But this IDEA of gene therapy brewed like coffee is hype. And frightening as all get out. Even if you thought mRNA/siRNA/CRSPR technology was safe and effective. EVEN THEN.
These issues I have delineated have not been examined or even thought about in this paper. There is one research pharmacist on this long list of authors. And I don’t know if he has personal experience within a hospital pharmacy. But there is a push to do this type of “compounding” because much of the biotech revolution/gene editing is a personalized N-of-1 manufacturing. And biotech cannot do this at a reasonable price. Furthermore, people/patients/governments will demand it.
Oh in case anyone is wondering what this NANOSPRESSO really looks like, here it is.
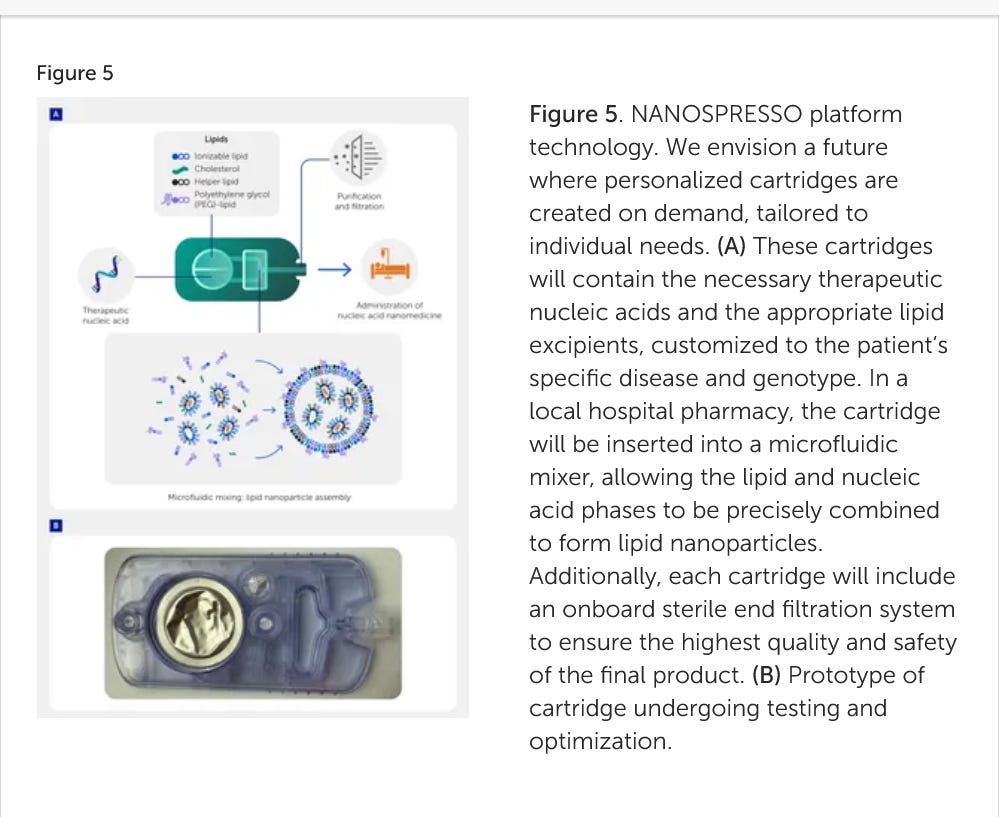
THAT’s IT?
I cant even say Holy Toledo.
Continue to pray the rosary. Always.
"Why are they doing this?" because they can, if nothing else during the farcical pandemic they have set the precedent for indiscriminate experimentation on humans without a mass uprising and they have got away with committing this crime with no punishment. The unacceptable has been normalised and no one seems willing to stand in their way, because of that they will continue to stretch the boundaries.
It's hard not to marvel at the immagination of these folks .... but like Iccarus ....I reckon their wings might melt ....just not on me thanks ....🤷🏻♂️🦧🤕🤦