
The Case for Antibiotics
A Stewardship Pharmacist makes the case for, and against antibiotics

A long time ago, in a galaxy far away, I was an expert infectious disease pharmacist. Drugs and Bugs. It was my specialty. I loved it. Hospital pharmacists are VERY GOOD at this. We get a ton of training on antimicrobials, how they work, how to dose etc etc. We also get a lot of training on lab work, monitoring and related topics including when to START and antibiotic and also when NOT to. This is more difficult than it appears.
So when I was asked “do antibiotics REALLY work?” and what hard evidence, i.e randomized, controlled trials (RCTs) are there that show significant measurable benefit? The literature seems to look only at symptom control and test of cure, and no mortality data. So what is going on? Can you address this and explain any underlying misconceptions and assumptions about bacterial infections?
But that is really 3 different questions.
do they work in severe, confirmed bacterial disease? (uh yes, dramatically)
do they work in mild, self-limiting or probably viral disease (marginally)
do they work in every patient regardless of host factors, environment etc? (no)
Here is my paltry attempt to briefly answer these questions. Let me start with a real live case that I was involved in.
The 22yo Man with Lemierre’s Disease
OK, so I was working in hospital until 2019, mostly as a consultant. But I was also spearheading the antimicrobial stewardship program at a small outlying community hospital which had little experience with clinical pharmacists. First thing in the morning I looked a the blood cultures (organisms found growing in blood) results. And my eyes popped out of my head. Fusobacterium necrophorum!!!. I went running to the ward. A 22-year-old with sore throat, and some unilateral neck swelling, and a fever and was admitted because he didn’t look well. The doc is thinking viral pharyngitis or peritonsillar abscess. I told him, ultrasound the neck, start him on piperacillin-tazobactam and get specialist help. He gets sent out to a tertiary hospital, has pulmonary septic emboli, needed a chest tube, that gets clogged, goes through hell, 4 weeks of antibiotics. Comes back to the peripheral hospital. His family tracks me down to thank me, because the doc told him, he is alive because I flagged Lemierre’s disease and got him on treatment fast enough. Another day or two of delay and the outcome could have been much worse. Before the development of antibiotics, this syndrome was common and had a fatal course within 7–15 days. And I think that is the only one of the 2 times in my 40 yr career that a doc directly acknowledged to the patient, that the pharmacist by flagging this rare disease saved the patients life. Well the antibiotics saved this man’s life. This disease appears to be increasing in recent years however. Here is an excellent review for those interested.1
Part I
The Epidemiological Triad: Why Infection Isn’t Just “Bug meets Human”
So who gets a bacterial infection? When does it happen? Why? How did this presumably 22 yo healthy male get Lemierre’s disease?
We use the epidemiologic triad as a heuristic. This concept began in plant pathology2 as the “disease triangle,” was adapted into infectious‑disease thinking in the early 20th century.3 Empirical outbreaks look at host, agent, and environment contributions, but it doesn’t always expain everything and its methodological limits have prompted critiques and modern refinements.45 Lets look at each leg of the triad briefly
THE AGENT
The agent in this case is the bacteria. Bacteria are real, observable, culturable, stainable organisms. See here,6 here7 and here.8 The latter article on the microbiome is a good one.
They can produce toxins
exotoxins (secreted proteins) such as tetanus toxin, botulinum toxin, diptheria toxin
endotoxins (lipopolysaccharides) the outer membranes of gram-negative membranes, released on bacterial death which drives septic shock
Some bacteria kill via toxins even after the bacteria is dead, you may need anti-toxins but you still need to stop the bacteria and stop it making toxins
virulence factors or what makes a bacterium able to cause tissue or other damage
capsules (evades phagocytosis)
biofilm formation (then antibiotics find it hard to penetrate)
enzymes like hyaluronidase, coagulase (can result in serious tissue damage like “eating” through heart valves)
innoculum size
some bacteria need lots of bacteria to cause disease
others are quite virulent like Shigella in which 10 to 100 organisms9 is sufficient to produce dysentry
antimicrobial resistance
TL;DR would take forever to explain but some antibiotics do not work for certain bacteria even from the first use (intrinsic resistance) and some bacteria develop resistance with exposure to antibiotics (inducible resistance)
Not all bacteria are created equal
always pathogenic (the invaders): tuberculosis, anthrax, Neisseria meningitidis
opportunistic (the dual-agents): these colonize you but cause disease and need treatment if host barrier breached such as S pneumonia, E coli, S aureus, and like in my guy above F necrophorum
never pathogenic (commensal only or the permanent residents): S epidermidis, almost never require treatment (ok we treat S epidermidis but only under specific host conditions e.g. if there is infected hardware)
toxin producing (tetanus, botulism, diptheria)
THE HOST
microbiome integrity: the commensal ecosystem that competitively EXCLUDES pathogens and keeps the dual agents in check, maintains mucosal barriers, helps with immune function
disrupted by antimicrobial use itself (THE PARADOX!), also proton pump inhibitors, hospitalization, chronic disease, hospitalizations
the host “breaks” from viral infections causing mucosal breaches, or from chemotherapy, diabetes, extremes of age
immune competence
neutropenia (low neutrophils), other immune defects (like complement etc)
age
the U shaped curve with children having immature immunity and the elderly with immunosenscence at highest risk
nutritional status: the historic link between famine and epidemic infectious mortality
THE ENVIRONMENT
Sanitation and clean water: the SINGLE BIGGEST population level intervention but doesn’t eliminate the need for antibiotics IF infection occurs
Crowding: military barracks, prisons, refugee camps, schools
Healthcare access: delayed presentation allows higher bacterial load and worse outcomes
Iatrogenic factors: hospitals put in central lines, ventilators, surgery, immunosuppressant drugs
Seasonality: flu in winter, etc
Since each host is different, each bug has its own virulence and pathogenesis, and environments differ, a bacterial infection is really an individual event. No two infectious processes in a patient is quite the same.
Part II
Most Bacteria Are NOT Contagious
One important point often missed in public discussions of bacterial infection is that most serious bacterial infections are not caused by external invaders that you “catch.”. They are caused by organisms ALREADY LIVING IN OR ON YOU, in your own skin flora, your gut bacteria, your oral commensals. Streptococcus pneumoniae lives quietly in the nasopharynx of healthy adults. E. coli lives peacefully in the gut until it ascends to the bladder or kidney. Fusobacterium necrophorum, the organism that nearly killed my 22-year-old patient, almost certainly came from his own mouth. What changed was not the bug. What changed was the host. A previous viral infection, a mucosal breach, a moment of immune vulnerability (like running a marathon, or not enough sleep) and a commensal (or colonizer) becames a killer. This is why the epidemiological triad matters so much. And it is why antibiotics, when they work, are not simply killing an invader. They are restoring the epidemiological triad that the host temporarily cannot maintain on it own.
Most infections are endogenous (like my example of Lemierre’s disease) and include
urinary tract infections
cellulitis (infections of the skin)
tooth abcesses and decay
sinus and ear infections
most pneumonias
Colonization is normal
Host factors trigger disease (a scratch, mucosal break, a previous viral infection, etc)
Antibiotics allows the host, who is temporarily overwhelmed, to restore equilibrium between his/her microbiome and the environment. Antibiotics do not work solely on their own. So if the host cannot help mount a sufficient immune response (like neutropenia caused by chemotherapy, immunoscenescence in the elderly, multiple previous infections treated with antibiotics, etc) then it is difficult for antibiotics on their own to eliminate the pathogen.
Truly Contagious Bacteria
Having said that, there are SOME bacteria that are truly contagious. That is they are not commensals or do not normally colonize you. These include:
Bacteria which cause pneumonias
Mycobacterium tuberculosis: TB is genuinely contagious, requires inhalation of bacilli from another person and close prolonged contact, though most people get latent TB and the infection is contained.
Mycoplasma pneumoniae: i.e., walking pneumonia, genuinely transmitted person to person (see this outbreak in 1978)10
Bacteria causing meningitis
Neisseria meningitidis: droplet transmission, genuinely contagious though it requires close prolonged contact
(note: pneumococcal meningitis is not contagious)
Other respiratory
Group A Streptococcus pharyngitis: genuinely contagious, hence school outbreaks
Bordetella pertussis (whooping cough): highly contagious
Waterborne/Foodborne
Salmonella, Shigella, Campylobacter: but how sick you get is based on the host response
Typhoid, Cholera
Sexually transmitted diseases
Chlamydia
Gonorrhea, Syphilis
which is why a patient history is so important in diagnosing infections. Most people in North America will never get infected with these agents (except maybe the foodborne illness), and only whooping cough and N. meningitidis have vaccines BTW.
A Note on Bacterial Pneumonias
Bacteria pneumonia is worth its own brief discussion because this is where issues with contagiousness, identification and treatment is tricky and a bit of a rabbit hole.
First, the diagnosis itself is HARD
Pneumonia is generally diagnosed as fever, cough and changes on chest X ray suggestive of an “infiltrate.” You also look for shortness of breath, elevated white count, pleuritic pain (pain on inspiration). However, these symptoms are not specific for pneumonia. It could be atelectasis (alveoli in the lung collapses, often seen after surgery), pulmonary edema (heart failure, fools even the best docs), pulmonary embolus, lung cancer, pneumonitis (inflammation but without bacteria as a cause), etc.
Second, finding the causative pathogen is also difficult
Even with diagnostics like blood cultures, sputum cultures, urinary antigen tests, PCR and next generation sequencing (NGS), a causative agent is identified in less than half of all community acquired cases.11 (and more viruses than previously thought). Only with multiplex PCR and NGS do you get close to 75% 12and that, only in a research setting. Strep pneumonia is still the most common cause, as it was at the dawn of the antimicrobial era.
Why is it so hard to find the pathogen then?
patients get antibiotics before cultures are taken
expectorated sputum (getting the patient to cough up from the bottom of the lungs) is often contaminated with bugs from oral flora
some organisms dont grow easily on standard culture media (like mycoplasma, legionella and TB)
there may be co-infections (viral and bacteria)
it may be polymicrobial (though I am doubtful of that unless the patient has frank aspiration of bowel contents etc)
Third, “bacterial pneumonia” is not one disease
It is a clinical syndrome caused by at least a dozen different organisms with completely different transmission routes, virulence mechanisms, and natural histories. In fact, taking a good history from the patient (how it started, what they were doing, anyone else sick, current medical problems) predicts the causative organism not infrequently. Step pneumonia is usually endogenous, BUT it can spread via droplets as well. It presents classically with a single rigor and pleuritic chest pain. This organism is also carried asymptomatically in 5-70% of health adults. Mycoplasma pneumonia is spread via droplets person to person, but there have been outbreaks in summer camps. Klebsiella pneumonia is also endogenous and is classically seen in alcoholics who aspirate their gut flora. Staphylococcus aureus (NASTY!) in also endogenous, and usually found post-influenza superinfection. Finally there is Legionella pneumonia which is spread through the environment (i.e. water) and NOT person to person or is endogenous. So not all pneumonias are contagious, many are endogenous from our own microbial flora, and some come from your water tap.
Fourth, the interesting one: Legionella
Legionella pneumonophila is a bacteria and accounts for about 4.6% of all community acquired pneumonias globally13, and upto 12.6% when modern combined diagnostics are used. It is never transmitted person to person, and does not normally colonize you or live on your body. It lives in water systems, cooling towers, hospital plumbing, hot tubs. The environment is the exposure in this case. Antibiotics (azithromycin, fluoroquinolones) address the agent. So respiratory contagion is not necessary for a bacterium to be lethal or to cause pneumonia.
And that is why pneumonia diagnosis and management is HARD, and why antimicrobials are both over- and under used for pneumonia.
Part III
The Pre-Antibiotic Baseline: What Happens Without Treatment
Let’s look at the natural history of untreated disease documented from the pre-antibiotic era. I used to give this anecdote from the first civilian (Albert Alexander) treated with penicillin in 1945 to all my pharmacy residents. He had cut his cheek from schrapnel he had septicemia, endocarditis (heart valve infection), osteomyelitis (bone infection) etc. He was at deaths door. They gave him small amounts of penicillin and he recovered within 48hrs. Unfortunately they did not have enough (even used his urine to recycle the penicillin) and he died at aged 42. You can read about it here.14
Documented Natural History
Pneumococcal Pneumonia
pre-antibiotic mortality was 30% in hospitalized patients15
modern treated mortality is about 1% in young and 5-15% in the elderly
still the most common cause of bacterial pneumonia world wide
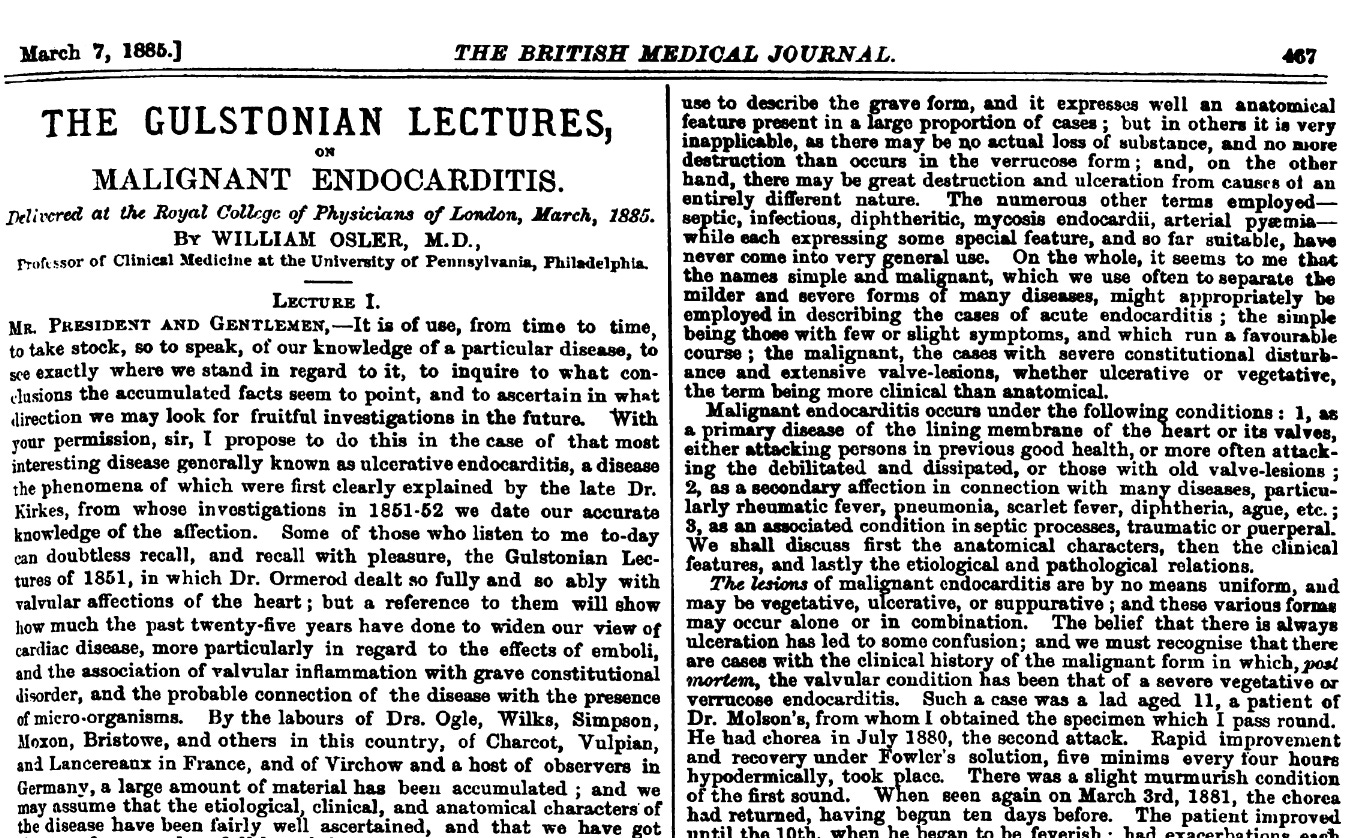
Bacterial Endocarditis
modern treated endocarditis has a mortality rate of 17%17 in a meta-analysis, varies by bug and region.
Here is William Osler lecturing on endocarditis in 1885 in the British Medical Journal. It is absolutely horrific.
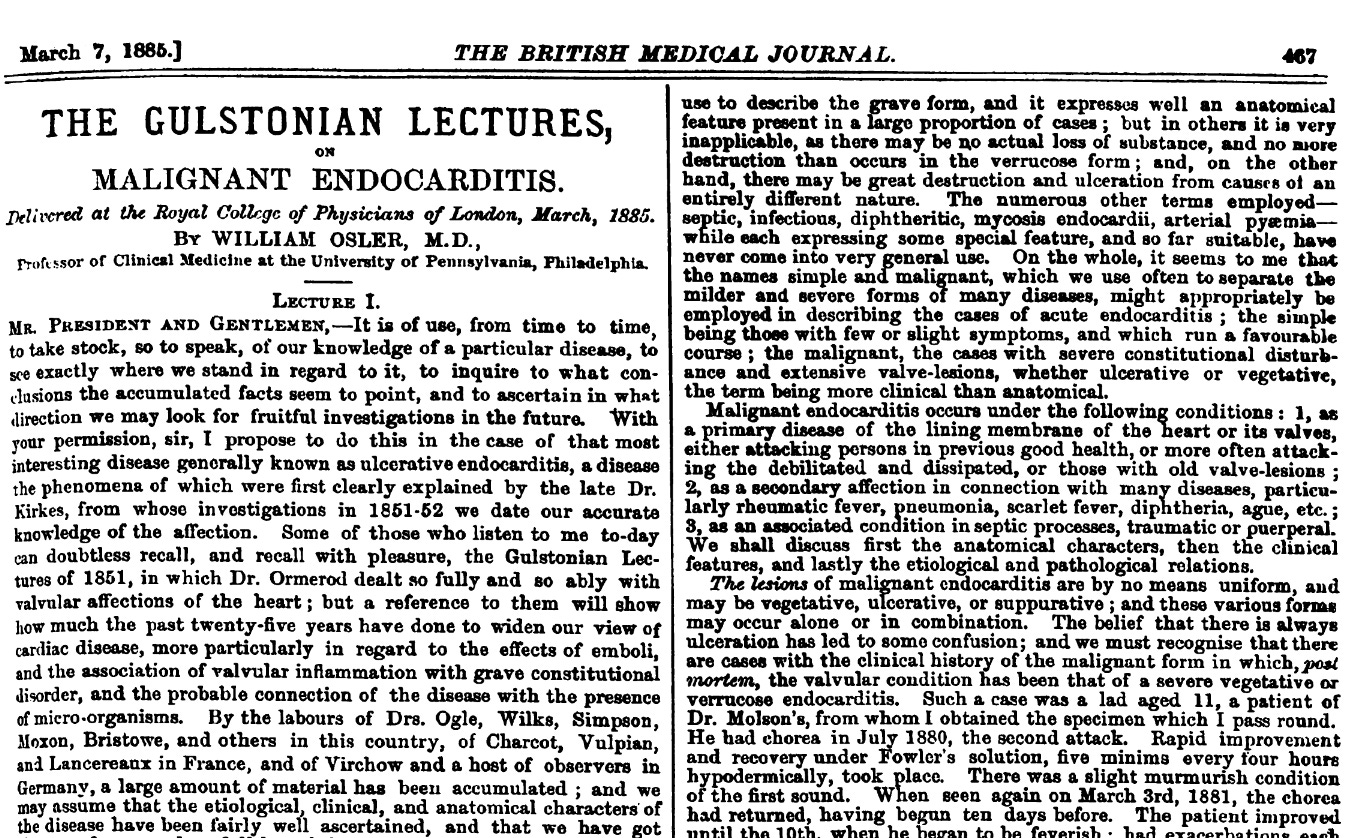
I have seen some of those complications Osler talks about even today. Endocarditis itself has not changed. But we have antibiotics and importantly, surgery to replace damaged heart valves. Today, a proportion of endocarditis arises from intravenous drug use due to contamination of the drugs, needles, other factors.
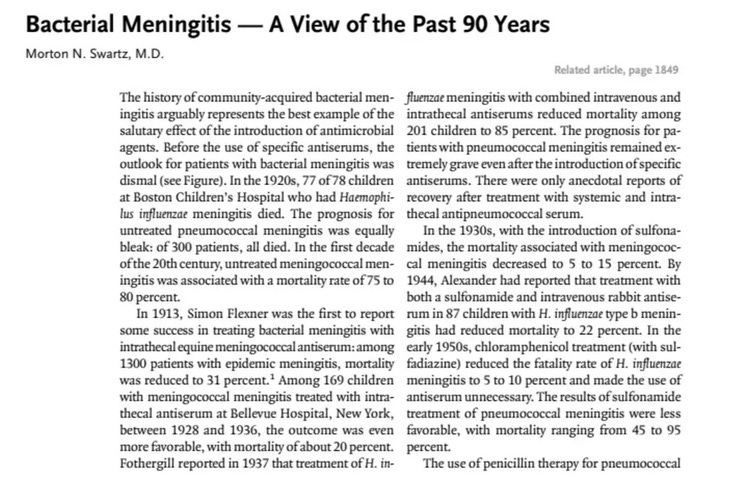
Bacterial meningitis
pre-sulfonamide treatment, mortality was about 75-80%18 Sulfonamide antimicrobials became available in the mid-1930s.
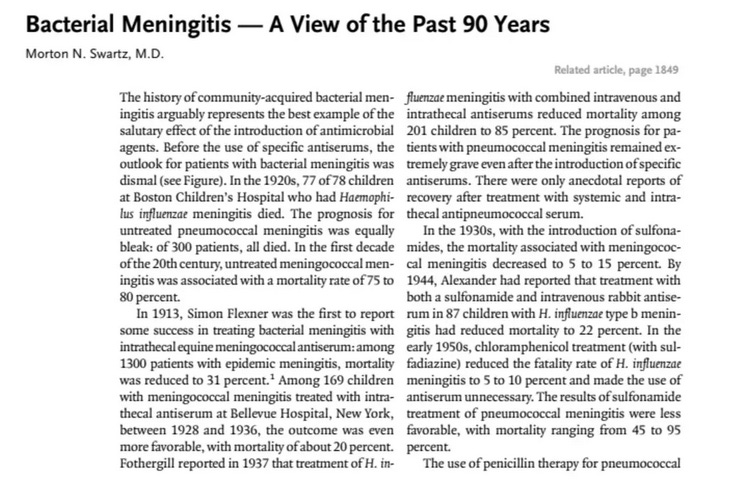
modern treated meningitis is still pretty bad but is about 5-15% depending on the bug19 and now we are adding corticosteroids to antimicrobials20, mostly Strep pneumo but also tuberculosis.
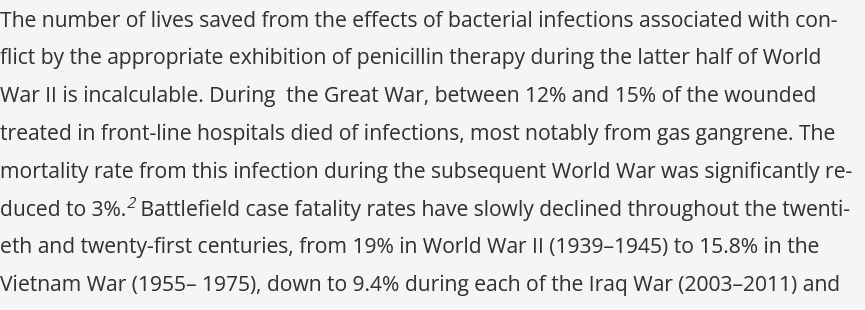
Infected War Wounds
now this is very very interesting and well documented21 especially about gas gangrene. We don’t see gas gangrene (Clostridium perfinges) much anymore, but I have seen a few cases and they are, shall we say, horrific as well.
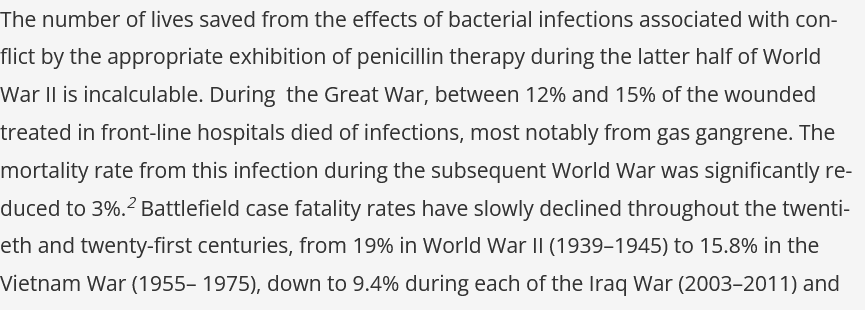
This historic review by Manring et al is well worth your time. Starting from the Greeks to modern warfare.22 Fascinating. Though surgery plays a large role in debridement of dead tissue, but that by itself is not sufficient, as the literature shows.
Acute Rheumatic Fever (ARF) Leads to Rheumatic Heart Disease (RHD)
this is a complicated infection. ARF occurs after Group A pharyngitis (infection of the pharynges or throat) in about 3% of people. Of that, about 60% develop RHD where you get heart failure from damage to your heart valves.
Group A Strep pharyngitis is common with millions of cases annually in children. Most resolve on their own. The host usually wins. But the risk compounds because there are over 200 M-protein serotypes of Streptococcus pyogenes. Infection with one strain confers immunity to that strain only. You can get strep throat again next month from a different serotype. Each infection is a new roll of the dice.
Therefore the individual risk per untreated infection is low and only 3% progress to acute rheumatic fever. But when you’re exposed to dozens of potential infections across childhood, the cumulative probability isn’t trivial.
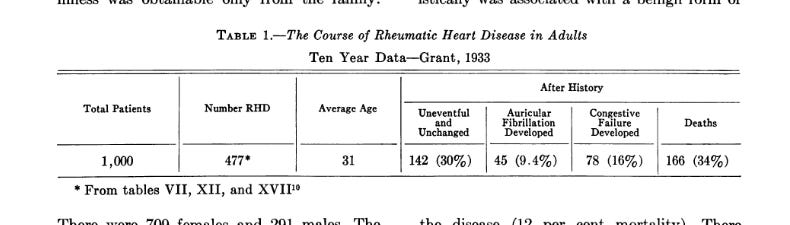
But once you’ve had ARF, the risk skyrockets. Without prophylaxis, recurrence rates after a new strep infection run 50% or higher. Each recurrence causes more valve damage. The Bland and Jones data below shows since the kids who did worst were the ones with multiple attacks.
Here is Bland and Jones in 195123 documenting 1000 cases in Boston between 1921-1931 of children who then developed RHD when there were no antibiotics and their outcomes as adults. Pretty sobering even though they say most patients did “fine.”
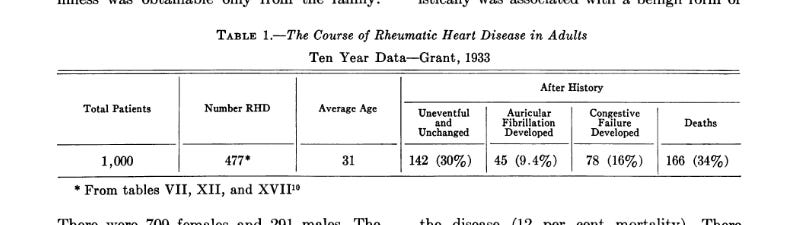
Lets just summarize this paper reviewing 1000 children.
301 out of 1000 dead within 20 years. That’s a 30% mortality rate in children and young adults from a disease that starts as a sore throat.
Of the dead, 80% killed by rheumatic fever and congestive heart failure. Their own immune systems, triggered by Group A Strep, destroyed their heart valves. This is the crazy part of ARF. It is an immune response to the bacteria.
Another 10% killed by bacterial endocarditis which Osler described as 100% fatal above, now layered on top of already-damaged rheumatic valves.
If you presented with a greatly enlarged heart or congestive failure early, you had an 80% chance of being dead within 20 years. As a kid.
And look how they described being sick with ARF was like for children.
Spent 3-6 months hospitalized, often 12-24 months
Had recurring attacks, 20% had another attack in the first five years, a further 10% in the next five years
Lived with the knowledge that any sore throat could trigger another round of valve destruction
Had no penicillin prophylaxis, no treatment for the initial strep infection, nothing to stop recurrences
This natural history described above was substantially decreased with penicillin.
Although ARF was the leading cause of mortality in 5‐ to 20‐year‐olds in the United States during the 1920s, the annual incidence of ARF in the United States today is low (<2 cases per 100 000 school‐aged children compared with up to 150 cases per 100 000 worldwide).24
A meta-analysis found antibiotics appear to be effective in reducing the incidence of acute rheumatic fever following an episode of suspected GAS pharyngitis. Here the number needed to treat was 53. So not as large an effect size as in endocarditis or meningitis but significant nonetheless25 because not everyone gets ARF.
Penicillin breaks the entire chain. Treat the acute pharyngitis and you don’t get ARF. If ARF does occur (say your Grp A strep throat was not treated), then you’ll receive monthly benzathine penicillin IM after ARF, and that results no recurrences. The bug never gets a second chance at the valves and you don’t develop rheumatic heart disease. (NOTE: benzathine penicillin availability is a mess. Pfizer has the market in the US and it is backordered for YEARS or is on allocation. The FDA allows imports from other countries because we cant make enough of a 70 year old drug. Don’t ask).
Others
Mastoiditis
Pre-antibiotics: 5-20% of acute otitis media progressed to mastoiditis
Mastoiditis mortality: 2-5% even with surgery; without surgery, much higher
Now: mastoiditis is rare enough that ENT (ears, nose and throat) residents may not see a case during training
Peritonsillar abscess (quinsy). This used to be quite common as a complication of untreated tonsillitis. This needs surgical drainage and can be fatal.
Lemierre’s syndrome caused by Fusobacterium necrophorum, “the forgotten disease,” now making a comeback. Almost universally fatal if untreated. See my experience at the start.
Brain abscess from untreated sinusitis (I had a case in an 8yo who had sinusitis for months, pain etc, parents were in the middle of a divorce and she was basically ignored. She seized and that’s when they found the abcess).
Orbital cellulitis from ethmoid sinusitis can lead to blindness, cavernous sinus thrombosis (I have seen this too)
Sepsis from pyelonephritis where E. coli in the urinary tract ascending to the kidneys and then to the bloodstream. This is quite common actually in post menopausal woman. Sepsis is bacteria growing in your bloodstream.
Part IV
The RCT Literature and What It Shows
The Ethical Constraints as Evidence
Here’s the problem. Those of us who have seen many infections up and personal and have used antimicrobials for cure, not just treatment, see the absence of placebo-controlled mortality RCTs as, well, not required. The need for antibiotics was answered so definitively be early observational data that further placebo-controlled trials become unethical.
This is what my profs said was the equipoise problem. Penicillin was shown to prevent rheumatic heart disease in observational studies, so no Investigational Review Board (IRB) would ever approve a placebo arm. Once streptomycin reduced tuberculosis mortality from 46% to 22% in the first year (see below) continuing to randomize patients to no treatment is seen as indefensible. (Oh, BTW, we need 3-4 drugs for 6-9 MONTHS to get truly rid of or cure TB, it is a nasty bug indeed).
So let’s look at the RCTs of antibiotics that are available.
Typhoid Fever (1948)
In 1948 Woodward and Smadel conducted a controlled trial of chloramphenicol for typhoid fever26 in Kuala Lumpur Malaysia. They treated 10 patients with chloramphinicol and compared them to 8 concurrent controls who received supportive care alone.
Treated group: 0 deaths of 10 (0% mortality)
Control group: 1 death out of 8 patients (12.5% mortality)
Here is what happened to the controls.
Fever for 35 days!! and then you die.
Here is an example of one patient who was treated with chloramphenicol, starting on the 6th day.
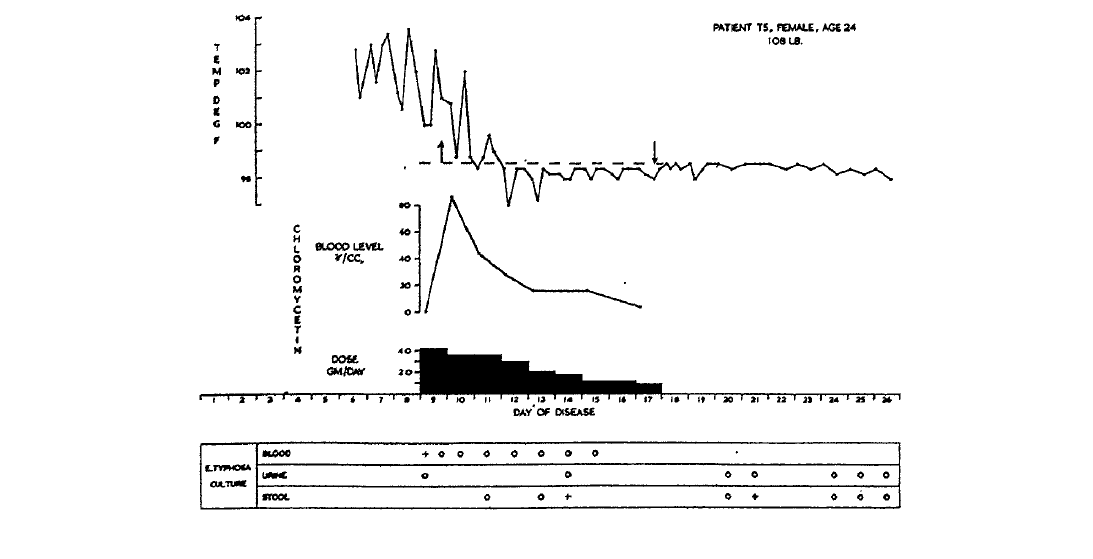
You can see a response to the fever by the 3rd day of treatment, and how they dosed the antibiotic in those days (high initial dose, then tapering off). Treatment for 9 days (is this where the default 7-10 days of therapy came from?) BTW, we dont use chloramphenicol anymore because it can cause grey baby syndrome in infants and a decrease in red blood cells in 1/3 of patients as well as aplastic anaemia (can be fatal).
The MRC Streptomycin Trial (1948)
The most famous RCT in history is the 1948 Medical Research Council (MRC) trial of streptomycin for pulmonary tuberculosis.27 The trial was designed by Austin Bradford Hill himself! The man who developed the criteria for causation that we use for when we can’t do RCTs or the effect size is great or for adverse reactions to drugs and vaccines.
Trial design: 107 patients with acute progressive bilateral pulmonary tuberculosis
RANDOMIZED (via sealed envelopes no less), AND a multicentre trial (across the UK) into:
a. streptomycin and bed rest (55 patients)
b. bed rest alone (52 patients)
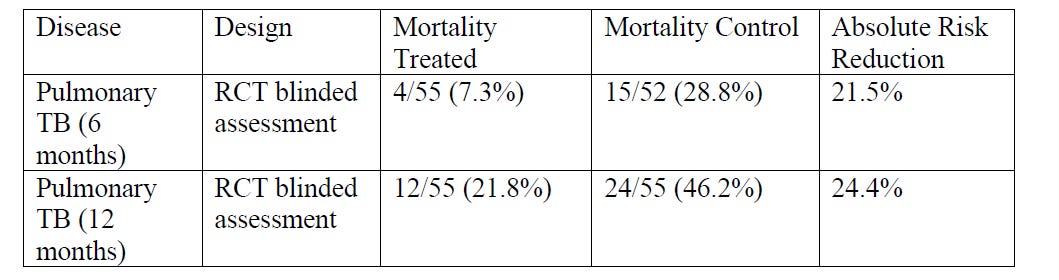
This is not subtle, and the treatment was in patients with advanced pulmonary TB. Today, we know that to eradicate TB we need 3 drugs for 6-9 months of therapy or more. TB is an ancient, tricky, horrible bacteria infecting over 2 billion of us (that we keep in check ie latent TB). Until we dont.
Time to Antibiotic Dose Response
Something that I see clinically over my 40yrs of practice about antimicrobial efficacy is the dose-response relationship between the TIME TO ANTIBIOTIC administration and mortality. This is why pharmacists are so very anal about this and ensure the antibiotic is available within 30 minutes or the order (only to have it languish on the floor for another hour or two. Sigh). This is because of a landmark study in 2006 by Kumar et al. and still behind a paywall. GRRRR. (personal note, Anand Kumar was an ICU resident/fellow when I was training in Winnipeg. Great guy and very sharp)
Kumar analyzed 2,731 patients with septic shock and found each hour of delay in antibiotic administration was associated with a 7.6% increase in MORTALITY. This dose-relationship is one of the gold standards of the causal inference in Bradford Hill’s criteria.
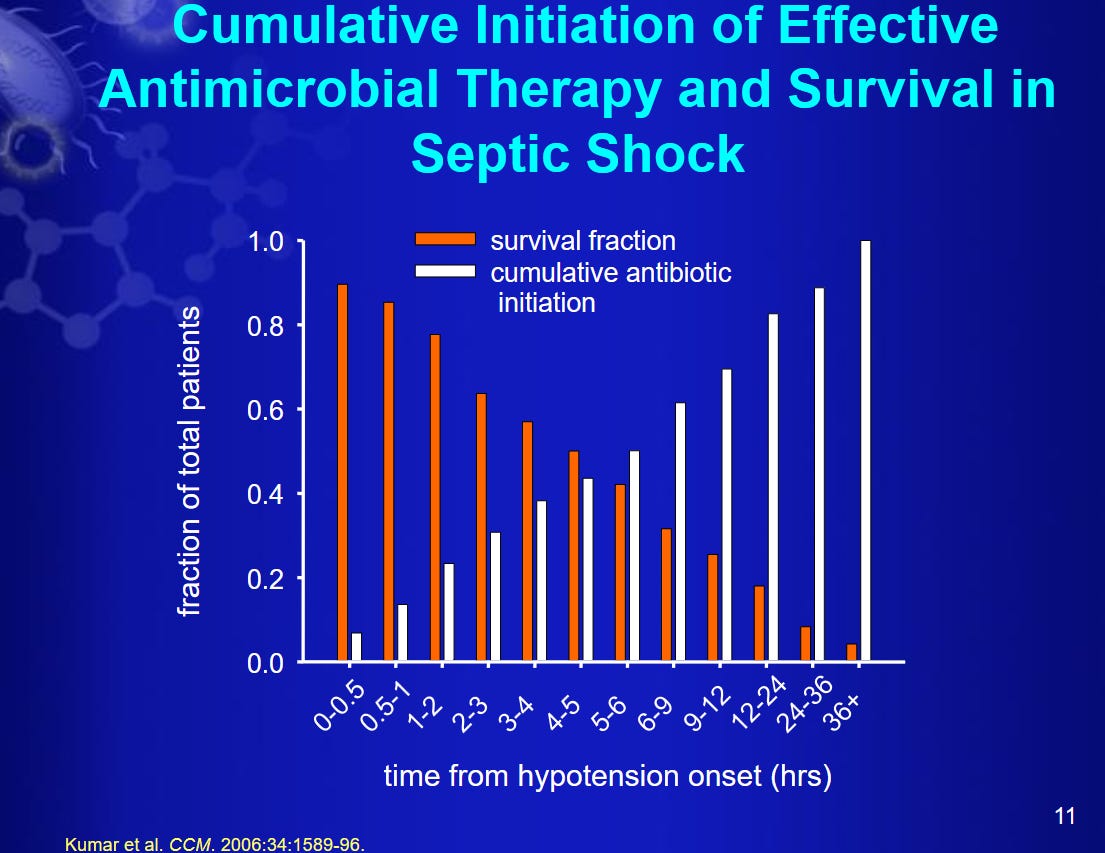
Above is from Anand’s presentation of his paper found here at a critical care conference in 2015.28 Some views on WHY time matters for sepsis in this presentation worth reviewing.
If antibiotics were just symptomatic timing wouldn’t matter. But EVERY HOUR counts in severe infections. This is not consistent with a placebo effect or spontaneous recovery.
Part V
Effect Size Matters
Not all drugs produce the same magnitude of benefit. Some interventions reduce risk by a few percentage points over decades. Others change the natural history of a disease so dramatically that the effect is obvious even without a large randomized trial.
This is one reason antibiotics occupy a unique place in medical history. The early successes of penicillin were not subtle, as discussed above. Diseases that had previously filled hospital wards and cemeteries suddenly became treatable. Pneumonia, bacterial meningitis, endocarditis, wound infections, puerperal sepsis, and many other bacterial infections no longer followed their known historical course.
The stronger the effect size, the less likely it is that bias alone explains the observation. This does not mean RCTs are unimportant. It just means that the amount and type of evidence required depends partly on the size of the effect being observed. A therapy that produces a dramatic and immediate change in outcomes can often be recognized with far less uncertainty than one that produces a small effect over decades.
Way back when, when evidence based medicine was in its early stages, there was a satirical paper on parachutes which made a serious epistemological point. We don’t randomize people to parachutes vs. no parachutes when we already know what happens without one. 29
This famous paper evaluated the effectiveness of parachutes. They found no studies, and used that to argue strict demands for RCTs can be absurd when the benefit of an intervention is glaringly obvious. The paper has become a classic citation in medical and scientific literature, often used to debate the ethics and limits of Evidence-Based Medicine (EBM).
And sometimes you CAN’T do RCTs, like for certain surgeries, medical devices or for serious adverse events. Use common sense. Not EVERYTHING needs an RCT (which has been corrupted by pharma in many ways over the ensuing years).
The effect size for antibiotics in infections are huge and imho, unambiguous. The only other medical case for which this kind of effect size of antibiotics has been seen is insulin for type 1 diabetes.
The Bradford Hill’s Criteria for Causation
So is observational evidence is sufficient for antibiotics and infectious diseases? Just to review here are the criteria (remember Bradford Hill30 designed the RCT for streptomcyin in TB trial).
Strength of association: The effect size of antibiotics on mortality in severe infections is enormous as discussed above (74% RRR in TB in the MRC trial).
Temporality: Clinical improvement follows antibiotic administration within hours or days (seen consistently like in the typhoid study)
Biological gradient: Dose response: higher bacterial loads benefit more; time to antibiotic shows dose response with MORTALITY, and not just symptoms or morbidity, as shown in the Kumar paper.)
Plausibility: The mechanism is established and uncontroversial. Antimicrobials kill or inhibit bacteria, reduce bacterial load and tissue damage.
Coherence: Laboratory, animal models, and clinical observation all align.
Experiment: Where ethically possible (mild infections, non-inferiority trials), antibiotics still outperform placebo.
Consistency: Observed across all settings, all eras, all bacterial infections
So what do you think? Is the effect size of antimicrobial therapy large enough we don’t need antibiotics? Has the Bradford Hill criteria been met?
Part VI
Evidentiary Tiers
With antimicrobial therapy you tend to have direct feedback loops (like you do with surgery or opioids for pain control). Lets look at some scenarios.
Tier 1: Antibiotics for Acute Infection
You treat. You observe. Within days to weeks (sometimes hours!), you know if it worked. The feedback loop is tight. When a patient with pneumococcal pneumonia goes from febrile and hypoxic to afebrile and saturating well in 48 hours, you’re not looking at a surrogate endpoint, in fact you’re watching the disease process reverse in real time. The causal chain is short and visible:
Antibiotic → bacterial suppression/elimination → resolution of infection (often alongside source control and host defenses) → survival
You don’t need an RCT powered for mortality when the natural history of untreated disease is known and the mechanism is directly observable. That’s why we say antibiotics are one of the few drugs which actually cure a disease.
Tier 2: Preventatives (Vaccines)
Here the feedback loop is loose to nonexistent. You give a vaccine to a healthy person. Nothing observable happens. Years later, they either do or don’t get a disease but you can’t attribute it causally in an individual case. The causal chain is long and invisible:
Vaccine→immune memory→?→no disease→?
The only way to evaluate this is population-level epidemiology with all its confounders. And the “hard outcome” demanded such as does this vaccine prevent death? requires massive, multi-year RCTs that are rarely done properly.
You can see an antibiotic work with your own eyes. You cannot see a vaccine “work” on an individual basis though I will acknowledge population-level signal for some vaccines is strong notably Hib meningitis near-disappearance31 (behind a paywall AGAIN!) since that vaccine was not available until the 1980s long after crowding, clean water, and better nutrition improved other infectious disease prevalence.
Tier 3: Chronic Preventive Drugs (Statins, Antihypertensives)
The feedback loop is delayed by decades. You give a statin to an asymptomatic 50-year-old. Nothing happens. Thirty years later, they do or don’t have an heart attack. The Number Needed to Treat (NNT) is huge. The individual patient never feels any different. The causal chain:
Statin→LDL reduction→slowed atherogenesis→?→fewer MIs
This is mostly dependent on surrogate endpoints (LDL, Total cholesterol etc) and long-term RCTs. When those RCTs are industry-funded and the absolute risk reduction is single-digit percentages, you’re right to be skeptical.
Part IV
When Antibiotics Are NOT Needed
Acute bronchitis in otherwise healthy adults: antibiotics don’t help. But if you have COPD, they do (here is where the host issues in the triad becomes important)
Most sinusitis: self-resolves; antibiotics provide marginal benefit. This is a hard one, because you get green yukky discharge, pain and fever and it seems you need antibiotics. Most dont as they are primarily viral though even bacterial sinusitis can be self-limiting, but as we saw previously you CAN get a serious infection from untreated sinusitis. This is where judgement comes in. Watchful waiting like for 2 weeks or so.
Many cases of acute otitis media: watchful waiting is appropriate in older children since many are viral. Again judgement and clinical expertise because some are bacterial and untreated bacterial otitis media can lead to deafness (which is what happened to my 96 yo mom. She had a sister who died of appendicitis too).
Asymptomatic bacteriuria (bacteria present but no symptoms): treating it is actively harmful (except in pregnancy)
Dental infections: source control (extraction/root canal) matters more than the antibiotic choice.
The overuse of antibiotics for viral syndromes and self-limiting bacterial infections has caused real harm such as C. diff, antibiotic resistance, microbiome disruption (the paradox). The medical establishment over-prescribes antibiotics. I have seen it often. Too often. Antibiotics are seen as benign or as insurance. But this does not mean antibiotic treatment is merely symptomatic.
The Resistance Angle
Antibiotic resistance is the strongest argument for judicious use, not for antibiotics are useless. Every unnecessary course erodes a shared resource. But this cuts both ways: withholding antibiotics when they’re indicated also causes harm.
The real scandal isn’t that antibiotics work, it’s that we’ve squandered them through agricultural use and lazy prescribing while the pipeline for new antibiotics has dried up because pharma can’t make money on drugs taken for 7 days versus drugs taken for life. And we are using antibiotics for 3-5 days and finding it is enough in most instances. My job was to make sure it was the RIGHT antibiotic for the RIGHT person for the RIGHT amount of time.
The Triad Revisited
Lets return to our opening framework. Antibiotics are a tool that addresses one leg of the triad. They’re extraordinarily effective at that one thing. But they’re not a substitute for:
Host resilience (nutrition, sleep, immune function)
Environmental improvements (sanitation, clean water, reduced crowding)
Source control (drainage, debridement, removal of infected hardware)
The best medicine addresses all three. Sometimes we think antibiotics will overcome the lack of host resilience, or that we can treat all diarrheal infections due to bacteria with antibiotics instead of clean water or in mild cases watchful waiting (and wonder why we have resistant Shigella strains).
Some caveats
This review is for bacteria ONLY. My knowledge and experience with viruses regarding pathogenesis, transmission etc etc is not that extensive since there really isnt much in the way of drugs or treatment out there. And I cannot comment on the diagnosis, transmissibility and pathogenesis of viral infections. Just don’t know enough. And I think viruses are fundamentally quite different from bacteria and we should not conflate the two as much as we do.
Surgery (and anesthesia which allows for surgery) plays a role in mortality in infectious diseases, especially for endocarditis and wounds of all kinds. I am reminded of a 51 yo male with diabetes visiting Winnipeg when I was training, who didnt show up to his sales conference to present his talk. He was found in his hotel room, unconscious. His blood cultures (3 out or 3) were positive for Staph aureus. At first we could not find a source. A few hours after he had his cardiac echogram which showed vegetations on his heart valve he acutely decompensated. His heart valve blew. He was in surgery for his valve replacement in less than an hour. THAT was what saved his life. But the antibiotics helped too lol.
Summary
I have spent forty years at the intersection of bugs and drugs. I have watched antibiotics pull patients back from the edge of things that, a century ago, would have killed them straight out, without ceremony. I have also watched them prescribed carelessly, for viral syndromes and self-limiting infections, or those best managed by incision and drainage. Both of those things are true simultaneously. Antibiotics are among the most important discoveries in the history of medicine. They are also tools that require judgment, restraint, and respect. They are not “free” and not without adverse events. But the evidence for their efficacy is not found only in clinical trial registries. It is found in the historical record, in the mechanistic science, in the patients who walked out of hospitals that their grandparents did not.
If we had applied current evidentiary demands to penicillin in 1942, we would still be waiting for THE definitive RCT on pneumococcal pneumonia.
I hope you get some indication of why I love bugs and drugs, and as always, continue to pray the rosary.
https://www.sciencedirect.com/science/article/pii/S1684118220300876
https://www.sciencedirect.com/science/article/pii/S2590346226001239
https://pmc.ncbi.nlm.nih.gov/articles/PMC3783101/
https://www.sciencedirect.com/science/article/pii/S2590346226001239
https://pmc.ncbi.nlm.nih.gov/articles/PMC10645024/
https://pmc.ncbi.nlm.nih.gov/articles/PMC10912505/pdf/fmicb-15-1370818.pdf
https://pmc.ncbi.nlm.nih.gov/articles/PMC7149789/pdf/main.pdf
https://academic.oup.com/cid/article/77/Supplement_6/S441/7459154?login=false
https://pmc.ncbi.nlm.nih.gov/articles/PMC4126259/
https://publications.aap.org/pediatrics/article-abstract/66/6/884/79271/An-Explosive-Outbreak-of-Mycoplasma-pneumoniae?redirectedFrom=fulltext
https://pmc.ncbi.nlm.nih.gov/articles/PMC7533148/
https://pmc.ncbi.nlm.nih.gov/articles/PMC8843176/
https://pmc.ncbi.nlm.nih.gov/articles/PMC8835084/
https://www.asbmb.org/asbmb-today/science/041722/guns-not-roses
https://pmc.ncbi.nlm.nih.gov/articles/PMC1555639/
https://pmc.ncbi.nlm.nih.gov/articles/instance/2255866/pdf/brmedj04768-0001.pdf
https://www.ajconline.org/article/S0002-9149(25)00110-9/abstract
https://www.ovid.com/journals/nejm/abstract/10.1056/nejmp048246~bacterial-meningitis---a-view-of-the-past-90-years?redirectionsource=fulltextview
https://pmc.ncbi.nlm.nih.gov/articles/PMC11297475/
https://pmc.ncbi.nlm.nih.gov/articles/PMC12889566/
https://pmc.ncbi.nlm.nih.gov/articles/PMC3013428/
https://pmc.ncbi.nlm.nih.gov/articles/PMC2706344/
https://www.ahajournals.org/doi/epdf/10.1161/01.CIR.4.6.836
https://pmc.ncbi.nlm.nih.gov/articles/PMC8475057/
https://pmc.ncbi.nlm.nih.gov/articles/PMC1164408/pdf/1471-2261-5-11.pdf
https://journals.sagepub.com/doi/epub/10.1580/1080-6032%282004%2915%5B218%3APROTBE%5D2.0.CO%3B2
https://www.jameslindlibrary.org/medical-research-council-1948b/
https://criticalcarecanada.com/presentations/2015/early_antibiotics_for_sepsis_and_septic_shock_a_gold_standard.pdf
https://pmc.ncbi.nlm.nih.gov/articles/PMC300808/
https://en.wikipedia.org/wiki/Bradford_Hill_criteria
https://pubmed.ncbi.nlm.nih.gov/8134226/
Comments are turned back on. Sorry.
Also, this post is a bit personal. I suffer from autoimmune neutropenia due to a drug I was taking for my rheumatoid arthritis. My bone marrow makes neutrophils but they get destroyed in my blood so my white count shows mild to moderate neutropenia. As a result I am at a moderately elevated risk for bacterial infections, and yes, I have had my share of cellulitis, and UTIs. These are all endogenous infections. So I am always scanning for bites, scratches etc and taking mannose for UTI prophylaxis. My risk for virus infections are low however.
From one pharmacist to another, thanks for this post! Infectious disease was a touch subject but quite interesting. I practiced community so not as specialized as the hospital, but that respect is still there.
You may appreciate my recent article on how to actually heal healthcare. I foresee we have a lot in common as we’re both off script. Here’s my recent piece if interested: https://unorthodoxy.substack.com/p/4-ways-to-save-healthcare-and-how