

1.Introduction
Can vaccines interact with drugs? Generally, the consensus is no. Drug interactions include
drug-drug interactions
drug-food interactions
drug-supplement interactions
In this case, interactions with vaccines would be classified as a drug-drug interaction. Now there are several MECHANISMS of drug interactions
pharmacodynamic: Pharmacodynamics describes the relationship between drug concentration and drug response.
interference with drug effects on receptor function (example: naloxone on opioid receptors since both compete for the same receptors)
interference with a physiological control process ( NSAIDs on the local prostaglandin E2 synthesis in the renal circulation decreases glomerular perfusion and increasing renin, thus ACE inhibitors don’t work as well)
additive or opposing physiological effects ( ex: combining benzodiazepines with alcohol is additive)
pharmacokinetic
absorption: interactions with absorption of the vaccine
distribution: competition for transport protein binding sites
metabolism: competition for the same CYP450 enzymes or inhibition or induction of specific enzymes
Elimination: competition for active transport, interference with solubility
Pharmacodynamic interactions are usually predictable based on the mechanism of action of each drug which is why you don’t drink alcohol and take a Valium.
Currently Drugs.com lists 345 drug interactions with the COVID-19 vaccines. Most of these are just known pharmacodynamic interactions; that is providing general advice if you are taking immunosuppressive drugs and the like. Personally, I find these kind of information useless as most are NOT clinically relevant.
Regulatory Requirements
Requirements? For Vaccines? Of course not. The EMA EPAR states


The only interactions that were considered were those with other vaccines, or how much reactogenicity was to be expected if you gave the mRNA COVID-19 vaccine and influenza vaccine together at the same time.
2. Clozapine: The first reported drug interaction with the COVID-19 mRNA vaccines.

In this report in 2021, a patient stabilized on clozapine for his schizophrenia, became acutely toxic 4 days after his Pfizer vaccine with a doubling of clozapine blood levels and requiring hospitalization. Since this patient was monitored closely, living in a group home and having his medications dispensed daily, the possibility of a drug interaction of the vaccine with clozapine was possible. Furthermore, he had an increase in the clozapine level previously with inflammation due to a pneumonia requiring hospital care.
An observational cohort study showed, yes indeed, clozapine levels can increase after COVID-19 mRNA vaccination, with some having levels high enough to be a concern for toxicity.
Antiepileptic Drug Interactions

In this case of antiepileptic drug interaction this review suggested that interactions were possible because antiepileptic drug interactions had previously been reported with influenza vaccines. A case of carbamazepine toxicity after influenza vaccination was reported. Serum levels of phenytoin (inc of 46-170%) and phenobarbital have been found to be increased temporarily after influenza vaccine. The authors warn this could happen with COVID-19 mRNA vaccines because influenza vaccine has been shown to increase interferon gamma production which down regulates the CYP450 system, specifically 2C19 and 3A4.
WHAT? These specific enzymes metabolize a whole slew of drugs and if influenza vaccination can affect this (albeit mildly) what about the super cytokine producing COVID-19 mRNA vaccines? This would mean the enzymes don’t work as well, and blood levels of certain drugs would rise, at least for a period of time until the inflammation is better.
A review paper found here
and an actual conference and minireview(Canadian researchers) reviewed the mechanisms of COVID-19 vaccines on drug metabolism.
The mechanism by which covid-19 vaccinations as well as the virus can affect a pharmacokinetic interaction is via inflammation down regulating CYP activity.

CYP450 drug interactions are the basis for most pharmacokinetic interactions. You have substrates then inhibitors and inducers and all sorts of mayhem can follow. For the most part, most interactions are not clinically relevant. Those that are usually include drugs with a narrow therapeutic index, ie. the difference between therapeutic level and toxic level is narrow. Such as clozapine above. If you want a quick and dirty overview here is a review article.
3. The Impact of COVID-19 Infection: CYP450 Down Regulation
So the actual MECHANISM of pharmacokinetic drug interactions with COVID-19 vaccines is the the pro-inflammatory response in COVID-19 infection, characterized by an increase in cytokines, such as C-reactive protein (CRP), tumor necrosis factor (TNF), interferon-γ, and a variety of interleukins including IL-6, reduces hepatic CYP3A4 metabolism resulting in altered drug levels and in some cases adverse drug responses. The McColl article above postulates that the vaccine can cause a similar inflammatory response as the infection. And as we know, maybe even worse.
In the paper below, they just focus on ONE CYP450 enzyme CYP3A4 as a result of infection. Well CYP3A4 is notorious because a LOT of drugs are fully or partially metabolized by this enzyme, ie they are substrates. This includes antidepressants, statins, calcium channel blockers, benzodiazepines (midazolam), HIV drugs, montelukast (remember that one for later), anti-rejection drugs like tacrolimus, amiodarone, quetiapine, clopidrogel etc.

Here is a most interesting table from this article.

HOLY TOLEDO! what drugs do you see?
midazolam results clearly show that high levels of plasma CRP (a marker of inflammation) are associated with slower metabolization of midazolam by CYP3A (a lower OH-midazolam/midazolam ratio meaning less midazolam was being metabolized). In the Le Carpentier paper (which studied sick ICU patients) they went on the say
These results are clinically important and may explain potential delayed awakening sometimes observed in patients with COVID‐19 suggesting a slowed metabolism of anesthetic drugs in these patients.
tacrolimus levels were HIGHER after a covid infection (ie the infection inhibited the CYP450 enzyme resulting in higher levels). Note tacrolimus is primarily used for patients who have had kidney transplants.
lopinovir/ritonivir (an HIV drug) was higher the greater the amount of inflammation as measure by the CRP level (so inflammation inhibited the CYP450 3A4; more inflammation was worse)
So giving a vaccine which codes for the spike protein and which results in the similar or even greater inflammatory response might be expected to have similar drug interactions, don’t you think? I agree with the McColl hypothesis.
PS. just throwing it out there. Say you got the vaccine, and then the infection in those first few weeks and got very ill with high CRP levels. You need ICU and are given normal or slightly higher levels of a midazolam infusion. Yeah. Not good. And the patients were bolused every 4 hours, instead of titrated to response which would have resulted in less midazolam. Just speculation, but these types of not very well known drug effects could have played a role in midazolam oversedation. I also wonder about propofol and fentanyl as well.
4. Role of CYP450 in COVID-19 Vaccination and Drug Treatment
In this paper they look at COVID-19 Vaccination and ANOTHER CYP450, CYP2C9. CYP2C9 is the next more important CYP metabolizing enzymes next to CYP3A4, some would argue even moreso.

This paper reviews all the potential drug interactions with drug therapy for COVID-19 including vaccines and herbs.
With respect to the vaccine, they propose that the
The concurrent use of drugs metabolised by CYP2C9, both inducers and inhibitors, should be taken into consideration by healthcare providers, particularly in patients with COVID-19 who received vaccines. As mentioned earlier, CYP2C9 is responsible for anti-seizure or anti-epileptic drug metabolism. Potential interactions between COVID-19 vaccines and anti-epileptic drugs could occur after vaccination.
Here is a nice figure on what the vaccination can do with respect to inflammation and resultant effects that affect drug metabolism that expands on the one up above.
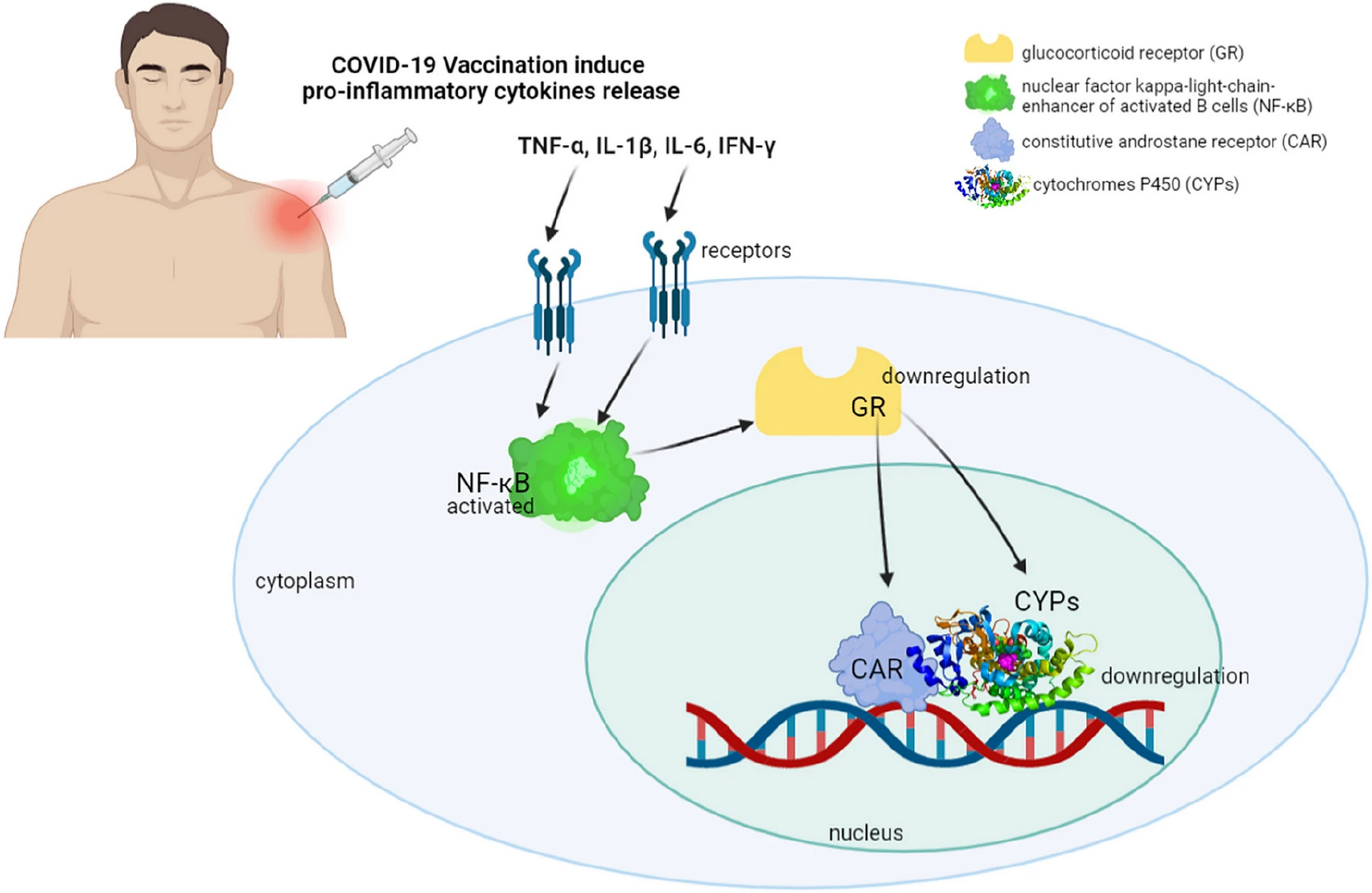
What is really interesting is that they propose that genetic variants of CYPs involved in pathologic processes, including the entrance of viruses into cells, anti-viral immunity and inflammatory response of COVID-19, are not entirely understood.
Considering the involvement of CYP2C9 and other CYPs in COVID-19 infection and drug metabolism, and the association of infection and inflammation with down regulation of hepatic and extra-hepatic CYPs, the genetic variability of CYPs across ethnicities could play a role in COVID-19 resistance and/or susceptibility.
Some of the drugs that have activity in COVID-19 therapy, or have potential activity are metabolized via CYP2C9 including:
fluoxetine
nirmatrelvir/ritonovir (Paxlovid)
remdisivir
omeprazole (Losec, a PPI)
montelukast (Singulair)
dexamethasone
ruxolitinib (Jakavi, a JAK kinase inhibitor)
statins
celecoxib (Celebrex)
herbs such as boswellia, quercetin, others
HMMMMM most interesting indeed. I think we are just scratching the surface here. Notice many of these drugs were used as TREATMENT for SARS-CoV2 ….could they have helped with dampening the effect of the vaccines if given at the same time? Thoughts?
5. Drug Interactions with the LNPs
So here we are going to talk more about the pharmacodynamic type interactions. For instance, WHAT ABOUT THE PHYSIOCOCHEMICAL NATURE OF THE LNPS? Are there any interactions in this respect? Well, this is where things get REALLY interesting.
Psychotropic Drugs
This very interesting article, which has been overlooked imho, critically reviews psychotropic drugs and how they can interact with the LNPs.
As we learned in my last post LNPs enter host cells via endocytosis or phagocytosis (immune cell endocytosis). LNP is trafficked through the endosomal-lysosomal system (ELS), traveling from early to late endosomes. Progressing from late endosome to lysosomes would risk LNP degradation; therefore, mRNA escape must take place in late endosome. (and no this is not the same Sabine as the microbiome doctor).
Ribosomal Function
They state several psychotropic drugs alter ribosomal function and protein synthesis such as
clozapine (we’ve already seen this!)
aripiprazole
lithium
chlorpromazine (inhibits mRNA expression in human thymocytes)
Upregulating ApoE receptors and/or increase LNP egress from cells
They could upregulate ApoE receptors, which would increaseLNP uptake into cells or increase LNP egress from the cytosol (ie exocytosis) Drugs mentioned include:
clozapine (again!!)
olanzapine,
haloperidol
aripiprazole
imipramine
trazadone
Increased endosomal escape
These authors suggest that the ionizable lipids likely contain synthetic polyamines which increase endosomal escape. This would include spermidine but not the tertiary amine on the LNPs. Spermidine WAS used in the in vitro transcription (IVT) of the mRNA1 and maybe some residual spermidine remains?
Novel studies attributed antipsychotic properties to spermine, while its dysfunction was associated with the pathogenesis of psychiatric illness, particularly suicidal behavior (Squassinaet al., 2013; Yadav et al., 2018). Moreover, as spermine plays a major role in male and female reproductive physiology, disruption of this polyamine may contribute to infertility and decreased birth rates (Lefèvre et al., 2011).
Say WHAT???? How much spermidine remains in these LNPs? At the present time I do not believe this is measured by the manufacturer or is included in the proposed compendial standards. Does anyone think this may be a problem?
So in general there is a lot of stuff going on in these patients on higher doses of antipsychotic drugs. Maybe they don’t respond to the vaccine that well or potentially if also on anti-epileptics have increased levels and increased adverse effects. It is interesting to note, that “vulnerable groups” included by the recent FDA recommendations for the jabs include those with depression or schizophenia spectrum disorders. These are the patients most likely to be on these drugs. (Note: to be fair, patients with schizophrenia were said to be at high risk for COVID disease before the vaccines were available, maybe partially due to the drugs they take and so more likely to be infected and with increased severity, though I am not sure if drug interactions were considered for the vaccine per se.)

And there is also chatter about antidepressant-vaccine interactions.
Drugs Which Help in Endosomal Escape
It is amazing to me how much money and time is being spent on improving the endosomal escape of the mRNA from the endosome. This is the bottleneck of the whole jabs. You would need a whole lot less LNPs (and presumably less AEs) if most of the LNPs actually do their job instead of just screwing up the cell membrane bilayer and accumulating in lysosomes causing lysosomal storage disorder-like effects among other things. However, since this is a very big topic I will leave it to another post.
SUMMARY
Drug interactions have been reported with COVID-19 mRNA vaccines, including those requiring hospitalizations
Drug interactions studies are not generally required for vaccines under current regulatory guidelines. This should be reassessed (for all vaccines, not just these mRNA jabs).
Classes of drugs most associated with drug interactions with the vaccine include psychotropic drugs and anti-epileptic drugs
Drugs metabolized through the CYP2C9 isoenzyme are of particular concern because if infected or given the mRNA vaccine the CYP450 enzyme is down regulated making drugs metabolized by this enzyme more likely to accumulate and make contribute to adverse events (and it would not be attributed to the vaccine because no one knows!). Drug and/or herbs metabolized by CYP2C9 have also been found to be helpful in the TREATMENT of SARS-CoV2 making this important to study and characterize.
If infected with the virus, CYP3A4 can be also be down regulated. Clinically relevant examples have been noted, such as tacrolimus, midazolam and lopinovir/ritonivir. A transient, but clinically relevent drug interaction to mRNA vaccines is also possible.
Drugs which affect endosomal escape are currently being studied in combination with the LNPs for better endosomal release. This is a very important topic and I will address this next.
And with respect to IVM, since it is metabolized via CYP3A4 and p-glycoprotein, drug interactions are possible but at therapeutic doses does not significantly limit the metabolism of other drugs. No interactions are reported on Drugs.com. Because of its high therapeutic index, significant clinically relevant drug interactions are unlikely.
Thanks for reading! I am not sure I did justice to this very important topic and would appreciate any comments or suggestions.
And as always, pray the rosary.
Uses of spermidine
Stabilizing Nucleic Acids: Spermidine, a polyamine, binds to negatively charged DNA and RNA, stabilizing the template DNA and newly synthesized RNA. This reduces nucleic acid degradation and improves transcription efficiency.
Enhancing Enzyme Activity: Spermidine interacts with RNA polymerase (e.g., T7, T3, or SP6 RNA polymerase commonly used in IVT), optimizing its activity and promoting efficient transcription.
Preventing Aggregation: It helps prevent the aggregation of nucleic acids and proteins, maintaining a favorable reaction environment.
Typical Concentrations: Spermidine is often included in IVT reaction buffers at concentrations of 1–2 mM, though optimal levels depend on the specific protocol and enzyme used.
My Dear Lady, if there was ever a pharmacist less washed-up than yourself, I have never met her. I am an old, retired pharmacist who has only in the last five years had time to read and study and actually learn something about viruses, vaccines and so on. Before that, I was just your typical allopathic Pharma parrot. Your articles leave me open-mouthed and in awe. Thank you and please continue.
Thank you for your informative post regarding the important interactions between clozapine, antiepileptics, and CYP3A4/CYP2C9 substrates, as supported by case reports and reviews. Enhanced monitoring and regulatory studies are essential to ensuring patient safety. However, I am uncertain whether institutions are wise to adopt these practices.